How do erections work?
Mechanism of penile function
Erection is basically a spinal reflex that can be initiated by the recruitment of:
- Penile afferents, both autonomic and somatic.
- Supraspinal influences from visual, olfactory, and imaginary stimuli.
Several central transmitters are involved in the erectile control. Dopamine, acetylcholine, nitric oxide (NO), and peptides such as oxytocin and adrenocorticotropin/α-melanocyte-stimulating hormone, have a facilitatory role, whereas serotonin may be either facilitatory or inhibitory, and enkephalins are inhibitory.
The balance between contractant and relaxant factors, controls the degree of contraction of the smooth muscle of the corpora cavernosa (CC) and determines the functional state of the penis. Noradrenaline contracts both corpora cavernosa (CC) and penile vessels via stimulation of α₁-adrenoceptors. Neurogenic NO is considered the most important factor for relaxation of penile vessels and corpora cavernosa (CC). The role of other mediators, released from nerves or endothelium, has not been definitely established.
In the flaccid state, the intrinsic smooth muscle tone and the sympathetic discharge exert a very high resistance to the incoming blood flow, thus the penis is in moderate state of contraction. When alpha-adrenergic agents such as phenylephrine, are injected into the corpora cavernosa, maximal contraction occurs and the penile shaft becomes shortened and firm.
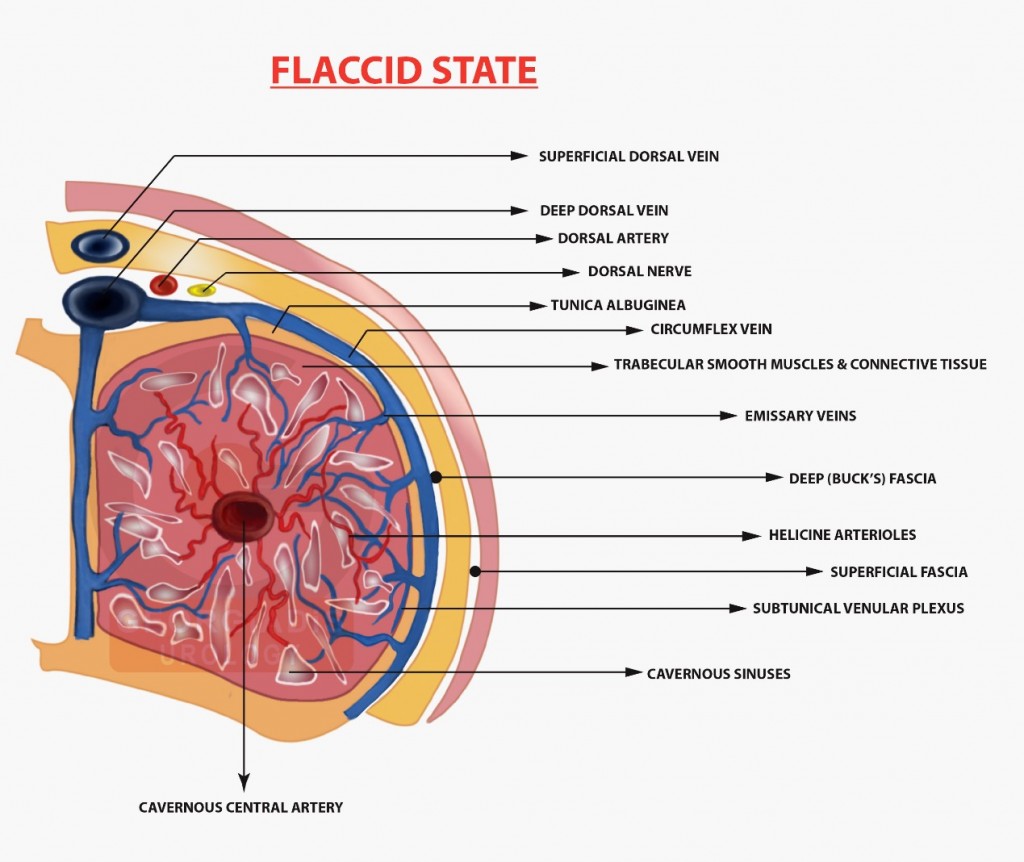
Figure 1: Graphical representation of the penile afferents during a flaccid state.
In the erect state, relaxation of the smooth muscles from neurotransmitters triggers the following:
- Increased compliance of the sinusoids and arterial wall, which lowers the resistance to blood flow to a minimum.
- Dilation of the arterioles and arteries by increased flow in both the diastolic and systolic phases.
- Trapping of the incoming flow by the expanding sinusoids.
- Expansion and elongation of the corpora cavernosa.
- Compression of the subtunical veins in the trabeculae between the tunica albuginea and the peripheral sinusoids, reducing the venous outflow.
- Stretching of the tunica albuginea encloses the emissary veins between the tunical layers with further diminution of the venous flow.
- Increased intracavernosal pressure up to 100 mm Hg as the result of increased filling, transforming the penis from the soft, dependent state to the erect, straight organ thus producing the full erection phase.
- Further increased pressure well above the systolic systemic pressure, as promoted by the stimulus that triggers the bulbocavernosus reflex thus producing the rigid erection phase.
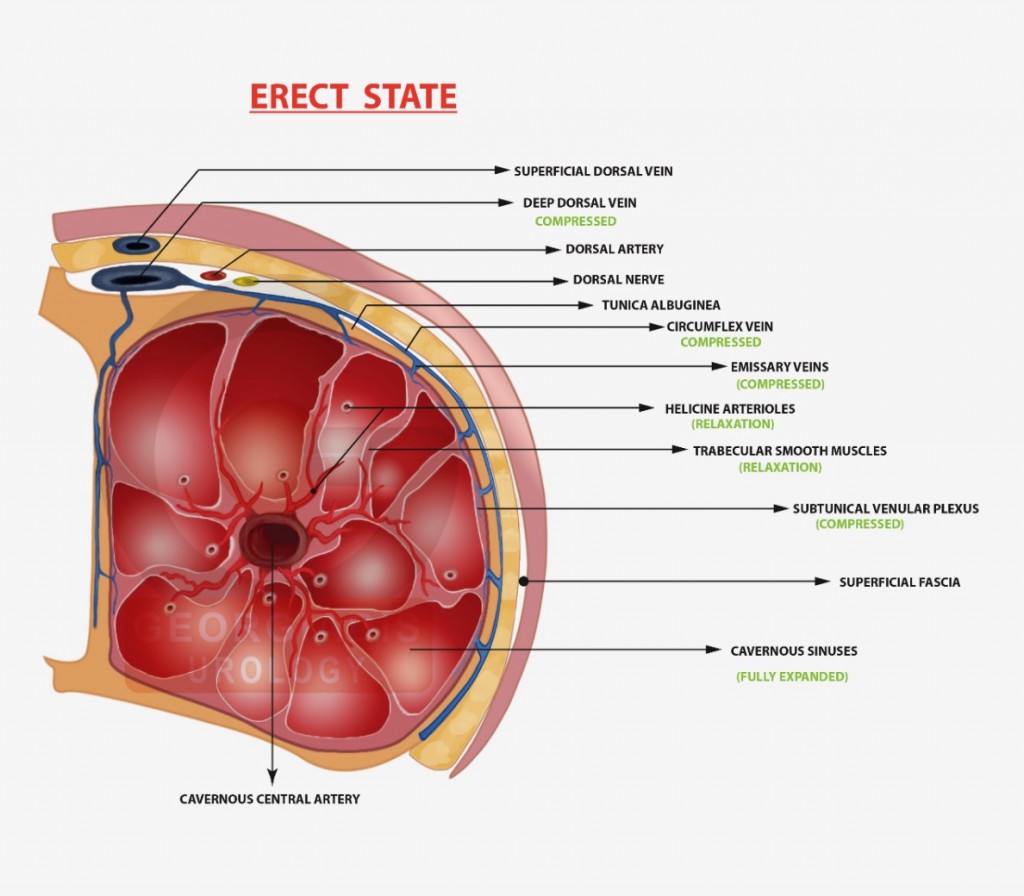
Figure 2: Graphical representation of the penile afferents during an erect state.
In other words, an erection involves sinusoidal relaxation, arterial dilation and venous compression, and occurs when blood fills two chambers known as the corpora cavernosa. This causes the penis to expand and stiffen, much like a balloon as it is filled with air. The process is triggered by impulses from the brain and genital nerves. Anything that blocks these impulses or restricts blood flow to the penis can result in erectile dysfunction.