
Chronic Prostatitis – Therapy
What is the treatment for Chronic Prostatitis?
This is obviously the most important, but also the most difficult part of a successful approach to chronic prostate inflammation.
To understand what I refer to as therapy is to understand the difference between radical treatment vs. simply decreasing or covering the symptoms for a finite period of time.
Great responsibility lies with the urologist, many of who typically attempt to downplay the severity of the condition – either because they have not made the correct diagnosis or because they simply do not know how to effectively treat the disease.
The goals of the therapeutic protocol should be nothing less than full and complete recovery:
- Complete elimination of the microorganisms that create the inflammation.
- Removal of the blockage in the veins of the prostate gland, the seminal vesicles and the epididymis.
- Removal of the purulent secretion and the micro-stones from the obstructed prostatic vesicles that cause inflammations.
- Recovery of the natural structure, size and function of the prostate gland.
- Complete elimination of the chronic prostatitis symptoms.
- Restoration and maintenance of physical strength, sexual capacity and fertility.
- Restoration and maintenance of psychological balance – the ‘feelgood’ factor.
Prostatitis effective treatment. Lasting recovery without relapse of symptoms.
The initial treatment of non-complicated chronic prostatitis begins with a course of antibiotics for a period of at least one month. This applies to cases where both clinical and detailed ultrasound examinations indicate the inflammation has progressed for a maximum of 6-9 months.
At this point we must be very careful to avoid loading the patient’s body with drugs without any practical effect. If follow-up clinical and ultrasound (and possibly microbiological) examinations show the inflammations persist – even in light of a partial or complete resolution of observable symptoms – the next stage of treatment will be more radical.
In my 25+ years of experience in treating chronic inflammations in the prostate, I have found that the only truly effective approach is a combination of antimicrobial and anti-inflammatory treatment together with finger compression gland therapy over a lengthy period of time. This therapy is adapted to the specific requirements of an individual patient’s inflammation.
The aims of finger compression gland therapy:
- Break the hard and organised foci of the inflammations in the prostate.
- Remove all the obstructions in the prostatic glandular ducts.
- Release strangulated nerves.
- Allow the smooth flow of the prostatic fluid on every glandular tube.
- Restore microvascular circulation in the glandular tissue.
- Remove all microbial cores.
- Restore a correct immune response to the healthy prostate glandular tissue.
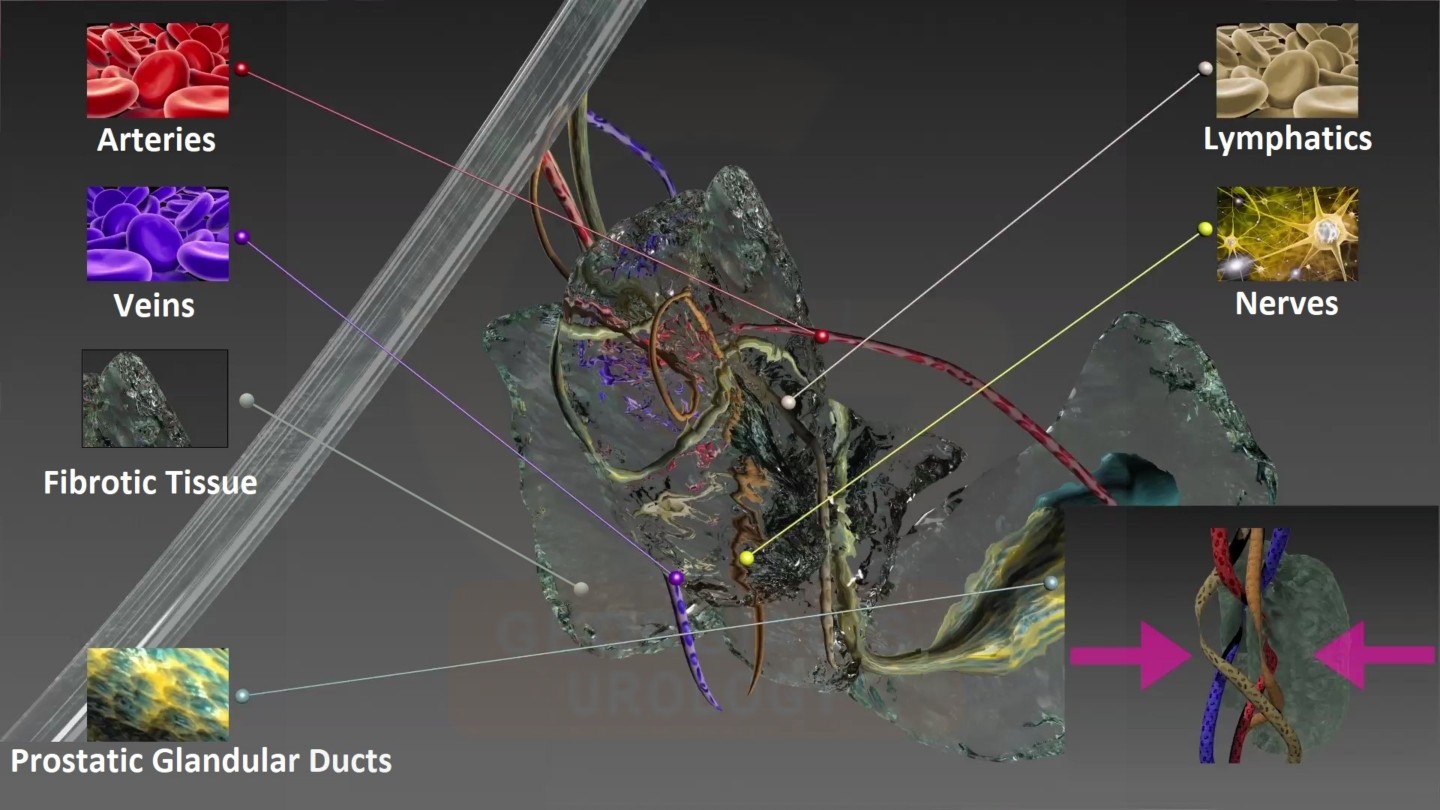
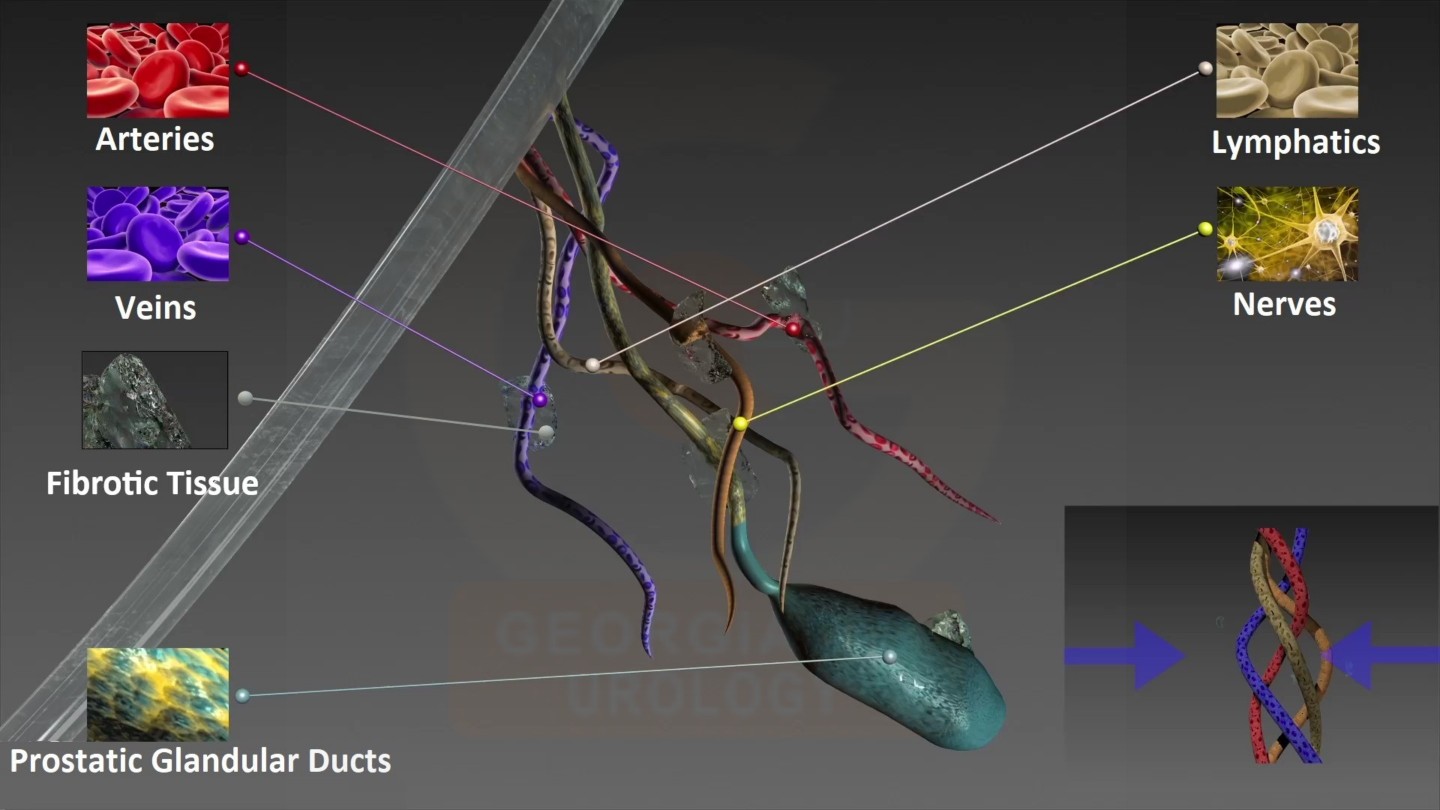
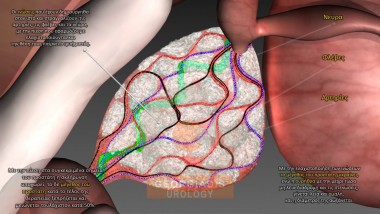
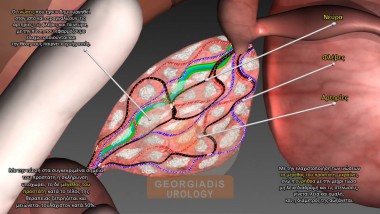
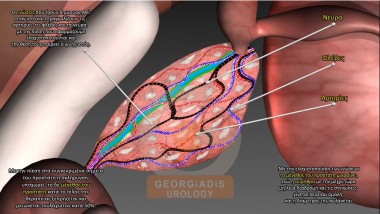
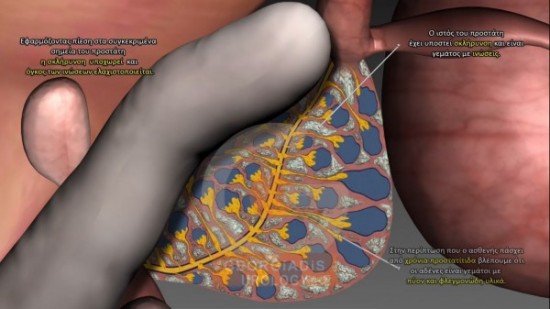
Figures 1 & 2: The first image represents a fibrotic prostatic tissue in Chronic Prostatitis patients, which strangulates the prostatic glandular ducts, the arteries, the veins, the nerves and the lymphatics. The second image represents the desired state of a prostate, which is what happens after applying the Georgiadis Chronic Prostatitis Protocol (GCPP). The fibrotic tissue has been almost cleaned up, which in turn achieves the aforementioned goals.
This chronic prostatitis treatment method delivers a highly impressive healing rate of 92%-96%.
It is based on the fact that:
- The prostate is gradually and carefully being treated area-by-area with every session through the rigorous and pinpointed prostatic pressures.
- This way the concentration of drugs in the prostate tissue can be multiplied by up to thousand times compared to oral ingestion leading to significant effectiveness in eradicating the microbes.
In a very few cases, typically less than 5%-6%, problems may persist:
- The symptoms of chronic prostatitis have not been fully eliminated.
- Microbes remain in the prostatic fluid culture after prostatic pressure.
- Microbes are eradicated yet leukocytes remain.
- The transrectal ultrasound identifies hotspots despite the complete elimination of germs and leukocytes.
- Multiple calcifications remain that may form microbes.
In any of these cases, I use intraprostatic and / or seminal intravesical mixture injections consisting of 4-5 antimicrobial and anti-inflammatory drugs in addition to the prostatic pressure protocol. The appropriate mixture is carefully selected per case based on an antibiogram following a thorough examination of prostatic fluid and sperm cultures.
Typically I perform one to three intraprostatic injections, each session separated by 15 to 20 days, which drastically improve the chances of definitive and lasting cure.
In the case where there are untreated leftovers, we risk a progressive worsening of the inflammation, resulting in the reappearance of symptoms and associated side effects (e.g. erectile dysfunction, infertility, urinary dysfunction etc.). These side effects are very likely to become the dominant problem that will ultimately cause the patient to visit the urologist for treatment again.
Georgiadis Protocol (Original)
The original protocol I developed for the treatment of chronic prostatitis is tailored for local residents and consists of the following stages:
Diagnosis: Before we begin the therapy we perform an extensive diagnosis (transrectal ultrasonography, urogenital ultrasound, uroflowmetry, microbiological exams etc.), and this is repeated in the middle and at the end of every stage.
First / Basic stage: The patient undergoes daily prostatic pressures for about 6 weeks. During this period the patient will be receiving the appropriate oral antibiotics (based on the symptoms, and the microbiological exam results).
Second stage: The patient then undergoes the same treatment for 10-20 prostatic pressure therapies every month for 3 months. This gives time for the prostate tissue to heal, and to help us see better the remaining inflammation points.
Third stage: If at the end of the second stage, there are indications of leftovers (e.g. inflammations, microbes etc.), we repeat a similar schedule as the second stage (i.e. therapies every month for 3 months), but additionally enhanced with intravenous along with intraprostatic injections in order to achieve radical and complete cure.
Georgiadis Protocol (International Patients)
For international patients (or patients who cannot visit Athens often), I have adjusted my protocol with the goal of achieving complete therapy in a shorter amount of time. The protocol is the following:
Diagnosis: Before we begin the therapy we perform an extensive diagnosis (transrectal ultrasonography, urogenital ultrasound, uroflowmetry, microbiological exams etc.), and this is repeated in the middle and at the end of every stage.
First stage: The patient has to come for 6 weeks, during which I will perform prostatic pressures twice per day. During this period the patient will be receiving the appropriate oral antibiotics (based on the symptoms, and the microbiological exam results) with 1-2 weeks of intravenous therapy (if necessary) and 1-2 intraprostatic injections (one in the middle and one at the end of this stage).
At the end of this stage, most patients will see an improvement of at least 70%-80%. The improvement will be objective (e.g. significant reduction in prostate size, reduction / eradication of microbe colonies, reduction of leukocyte count, improvement in the image of the prostate in the transrectal ultrasound and other exams, improved uroflow etc.) and in many cases subjective (e.g. symptoms may be eradicated or mostly alleviated). There are cases, where patients will experience significant objective improvement but they may feel that their subjective improvement is limited – this happens, because the strangulated nerves inside the prostate inflammation, even if the inflammation is 90% treated, the 10% leftover is still enough to preserve some noticeable and persistent symptoms. And at this point, I must stress the importance of the second stage, where the prostate has recovered significantly from the first stage and the patient is now ready to finish their therapy.
Second stage: About 1-2 months later, we perform all the examinations again and if the issues persist (e.g. indication of leftover microbes, inflammations etc.) we repeat the same protocol as the first stage for a period of 3-4 weeks (depending on the individual situation).
Note: I ask my international patients to come for six weeks to reduce the chances of leftover microbes (and hence the chance of relapse). Some patients may need only 50 sessions (e.g. 25 days), but some cases may need 70 sessions (e.g. 35 days) or even more OR they might need to visit me again a second time (for 10-20 or so days after a month or three months, it depends) OR they may need additional intraprostatic injections OR they may have symptoms (e.g. urethral stricture) that require extra work (as they naturally aid in microbe infections so they need to be treated). This depends on how long the patient has had the disease, the types of symptoms they have, the complications that have been established, the types of microbes and their resistances, and I cannot know in advance what each case will be. The aforementioned must be kept in mind before deciding to go through the protocol.
Finger Pressure Unblocking Prostate Therapy
One of the key aspects of the Georgiadis Protocol are the specialised prostatic pressures, which should not be confused with simple prostatic massages or anything similar.
The following visualisations aim to describe the technique and shed some light into the difference that I am referring to:
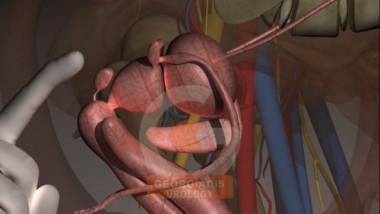

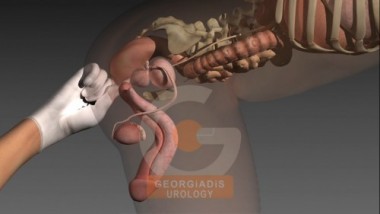
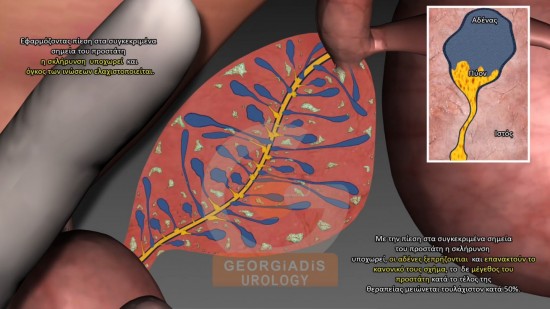
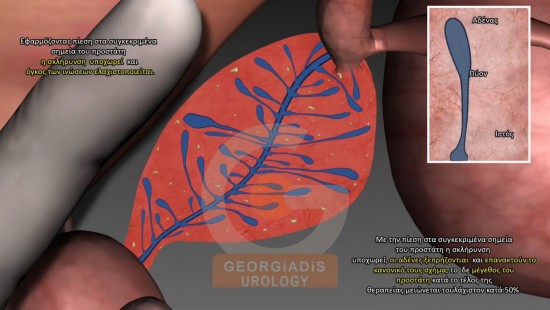
Figures 3, 4 & 5: Visual representation of the Finger Pressure Unblocking Therapy for the prostate. The pressures are targeted at specific regions each therapeutic session, they are thorough and rigorous. The targeted areas and the duration of the pressure depend on the inflammation, elasticity and hardness of the prostate tissue area.
Figures 6, 7 & 8: Through the stages of the Georgiadis Protocol, the fibrotic areas of the prostate are gradually being dissolved, the vessels are being released, the nerves are being unblocked and the prostate size is gradually reducing to normal.
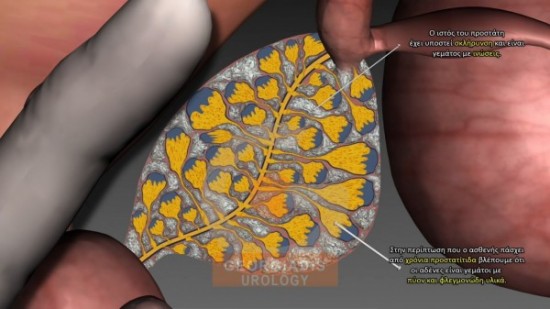
Figures 9, 10, 11 & 12: In addition to the aforementioned effects, the aim of the Georgiadis Protocol is to clear the prostatic glandular ducts from the puss and other inflammatory products. This may be the most beneficial and difficult part of the protocol, but is what ultimately leads to a full cure and what makes the defining difference with other techniques that claim to do something similar.
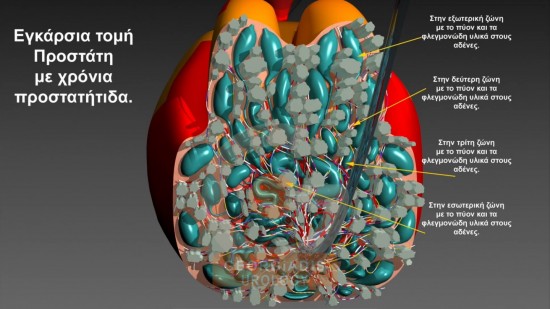
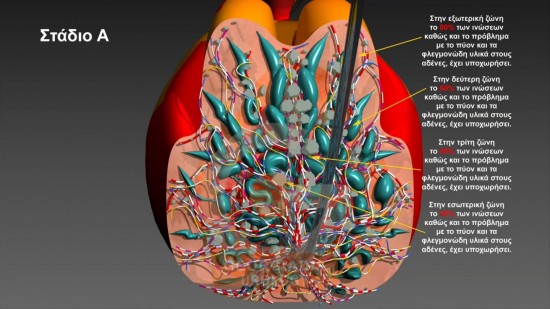
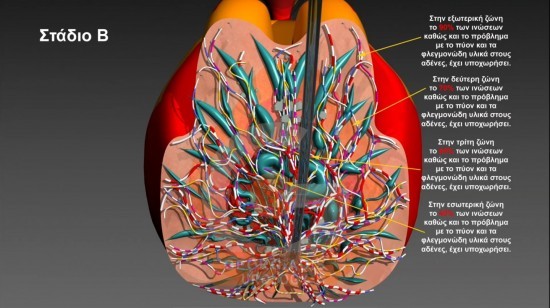
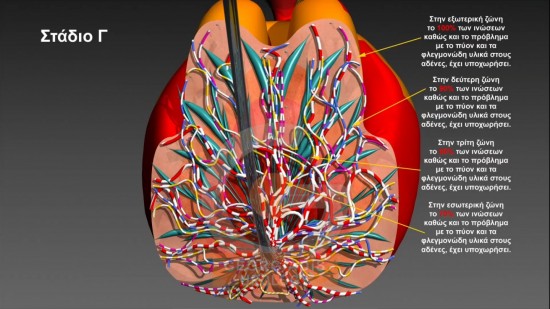
Figures 11, 12, 13 & 14: A 3D representation of the prostate state, from the beginning (when a patient typically begins the treatment), to the intermediate (typically at the end of the first stage of the therapy) through the final stage (which is full cure without relapse). To sum up, the effects are 1) removal of obstructions inside the prostatic ducts 2) release of stangulated nerves, vessels & lymphatics 3) smooth prostatic fluid circulation, which ultimately allows the medications as well as the body’s immune system to reach the areas of interest and 4) removal of all microbial cores.
Intraprostatic Injection Protocol
Intraprostatic injections-based-treatment offers an alternative to the complete digital rectal treatment for those who may be unable to follow the protocol such as:
- Patients with limited time due to work demands.
- Patients with high sensitivity to digital pressure.
- More mature patients above 60 years old.
A mixture of anti-microbial and anti-inflammatory agents, addressing the full range of microbes that potentially cause chronic prostatitis, are usually applied once a month for three to six months. In cases where the patient has been suffering from chronic prostatitis for a significant amount of time, say 20 to 25 years, or the prostate size exceeds 60-70 grams and displays advanced prostate tissue lesions. This may take up to 10 repetitions but usually about 6 are enough.
Every case differs but the patient who will follow this protocol will typically undergo 3-10 days of prostatic pressures before going through an injection (so that its effectiveness is optimised), and this will be repeated 3-4 times.
How the injections work
Intraprostatic injections are performed using a special transrectal ultrasound head equipped with a guide, allowing the needle to inject antimicrobial drugs directly into areas where major chronic inflammatory lesions of the prostate parenchyma are present.
Directly injecting antimicrobial drugs dramatically increases their efficacy by hundreds of times and multiplies their concentration and diffusion between 500-1000 fold.
The number of injections required is determined by studying images of the intraprostatic lesions, with a transrectal ultrasonography examination undertaken one month after each injection.
Immediate decrease in symptoms
The first intraprostatic injection will usually decrease symptoms such as pain, frequent urination, burning sensation during urination etc. by 40% to 50% as reported by my patients. This will be lower for more obstructive problems such as difficulty in urination. On average, 70% to 80% of patients see significant improvements after 3-4 injections.
Intraprostatic-based therapy represents a satisfactory alternative, yet it will not cure chronic prostatitis. Nevertheless, it delivers good results in addressing the major or persistent discomforts that affect quality of life. Overall, improvement rates are around 65% to 70%.
