
Sexual Dysfunction – Therapy (GERP)
Two-phase Protocol for Erectile Dysfunction
Any effective treatment of erectile dysfunction must be done as a two-stage process. There is a cause (i.e. Chronic Prostatitis), and an effect which then leads to permanent lesions in the penis (i.e. mild fibrosis-sclerosis of the cavernosal tissue). The latter is ultimately responsible for what the patient experiences with regards to most common erectile issues, but unless the former is combated, any methodology that would focus solely on the penile tissue would be in vain.
Phase 1 – Treating Chronic Prostatitis / Chronic Pelvic Pain Syndrome (GCPP)
So, the patient first has to treat the cause of the symptom, which is Chronic Prostatitis, and for that I practice the Georgiadis Chronic Prostatitis Protocol (GCPP).
The goals of the protocol are the following:
- Clear the prostatic glandular ducts from the suppurative inflammatory secretions. These secreations contain the microbes and the inflammatory products.
- Soften and clear the inter-glandular (stroma) tissue from the sclerotic-fibrotic lesions and microbes,
- Release the strangulated prostatic vessels and increase blood flow. This will increase oxygen levels, antioxidative agents, factors of the immunologic system and concentrations of antibiotics in microbial sites, in order to exterminate them.
- Deliberate the intraprostatic neural plexus which will progressively decrease the symptomatology.
- Release the fibrotic and sclerotic inflammatory periurethral tissue, transforming it into an elastic and functional soft tissue. This leads to improvement of the urine flow and progressively decreases the intraprostatic urine reflux.
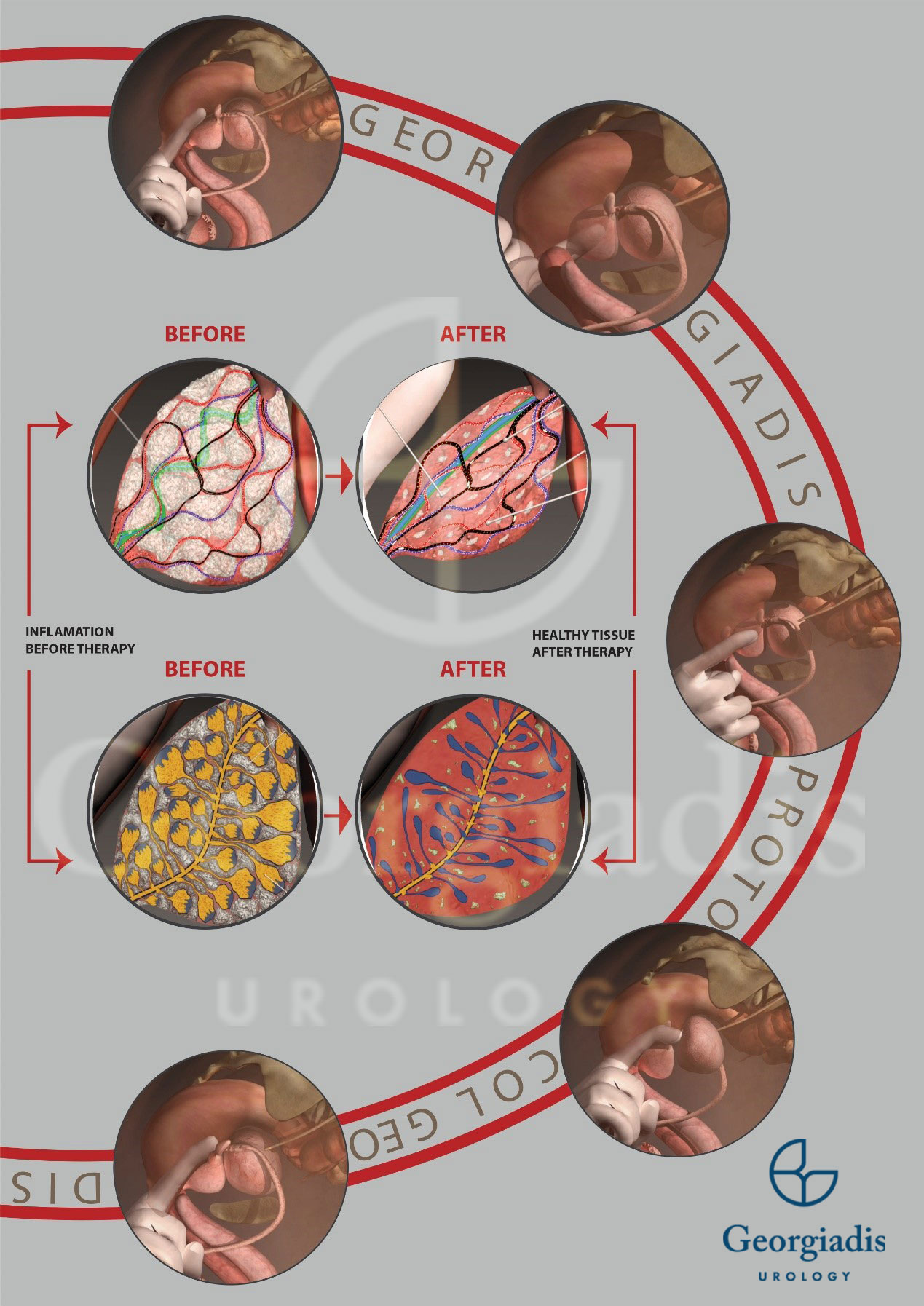
Figure 1: A visual overview of the Georgiadis Protocol for the treatment of chronic prostatitis. The prostate pressures are typically performed daily (or twice-per day), are rigorous and thorough.
When the patients have reached stages 2 or 3 of sexual dysfunction, they require additional work. Simply unblocking the nerves by treating and curing CP is not enough, but it is a prerequisite to proceed further. So, after usually a couple of weeks from the beginning of the Georgiadis Protocol therapy, I additionally begin performing supplementary treatments for the restoration of the cavernosal penile tissue.
For the readers who would like to know more, we have published an article on the mechanism of how Chronic Prostatitis contributes in erectile dysfunction in detail.
Phase 2 – Treating the Cavernosal Penile Tissue (GERP)
In order to restore the cavernosal penile tissue, I have developed the “Georgiadis Erectile Revivification Protocol” (GERP), which combines three therapeutic methods that happen at the same time:
1. Intracavernosal injections
Intracavernosal injections of vasoactive agents have long been recognised as a beneficial non-surgigal treatment for erectile dysfunction. Up to 15% of patients have reported return of erectile ability regardless of the causing factor after a course of intacorporal (i.e. intracavernosal) injection therapy.
Mechanism:
- Improved cavernous blood flow
- Improved cavernous oxygen concentration
- Mechanical dilatation of cavernous arteries and/or mechanical stretching of cavernous and tunical tissues.
- Improvement in tissue compliance and corporo-venous occlusive efficacy.
- Angiogenesis, neovascularization of cavernous tissue and hypertrophy of cavernous smooth muscle, all of which result in enhanced efficiency of the cavernous physiology.
2. Vacuum Pumps
Vacuum Erection Device (VED) is a useful noninvasive tool which can help in the treatment for erectile dysfunction. A vacuum erectile device, which mechanically creates penile blood engorgement, consists of 1) a vacuum chamber or cylinder, 2) a pump to produce negative pressure and 3) constriction rings. Once the cylinder is placed over the penile shaft, the pump is activated to create a vacuum inside the cylinder. As soon as the penis is engorged, the constriction band is pulled from the cylinder onto the base of the penis. The negative pressure is released through a valve and the cylinder is then removed.
Mechanism:
- Decrease in the hypoxic provocative factor (i.e. antihypoxic mechanism)
- Increase in the growth factor (i.e. antiapoptotic tissue mechanism)
- Increase in the smooth muscle-to-collagen ratio (i.e. antifibrotic mechanism)
- Upregulation of the endothelial’s nitric oxide synthase (NOS) expression (i.e. vasodilatory response)
3. Shockwave Therapy
Low-intensity extracorporeal shockwave treatment (LI-ESWT) is a modern therapeutic method for erectile dysfunction. It has been applied in my clinical setting in the recent few years with encouraging results.
Mechanism & tissue changes:
- Several studies showed that shock waves interact with the targeted (penile) tissue, initiating a cascade of biological responses. These responses include:
- Expressions of vascular endothelial growth factor (VEGF)
- Endothelial nitric oxide synthase (eNOS)
- Nerve growth factor (NGF)
- Neuronal nitric oxide synthase (nNOS)
- α1 & α2-adrenergic receptors (α1AR, α2AR)
- Tissue regeneration, neovascularization, angiogenesis and improvement of blood supply with new helicine arterioles and improved microcirculation.
- Reduction of inflammatory process and oxidative stress.
- Promotion of the regeneration of endothelial and smooth muscle cells, as well as triggering of anti-fibrotic effects.
- Recruitment of endogenous stem cells and nerve regeneration.
- Increase in the quantity of the smooth muscles and elastic fibers.
- Decrease in collagen and lipids.
- Tissue remodeling and elasticity restoration.
- Increase in the expression of α2-AR with a parallel decrease in the expression of α1AR. This results in decreasing the sympathetic nervous activity in the erectile tissue.
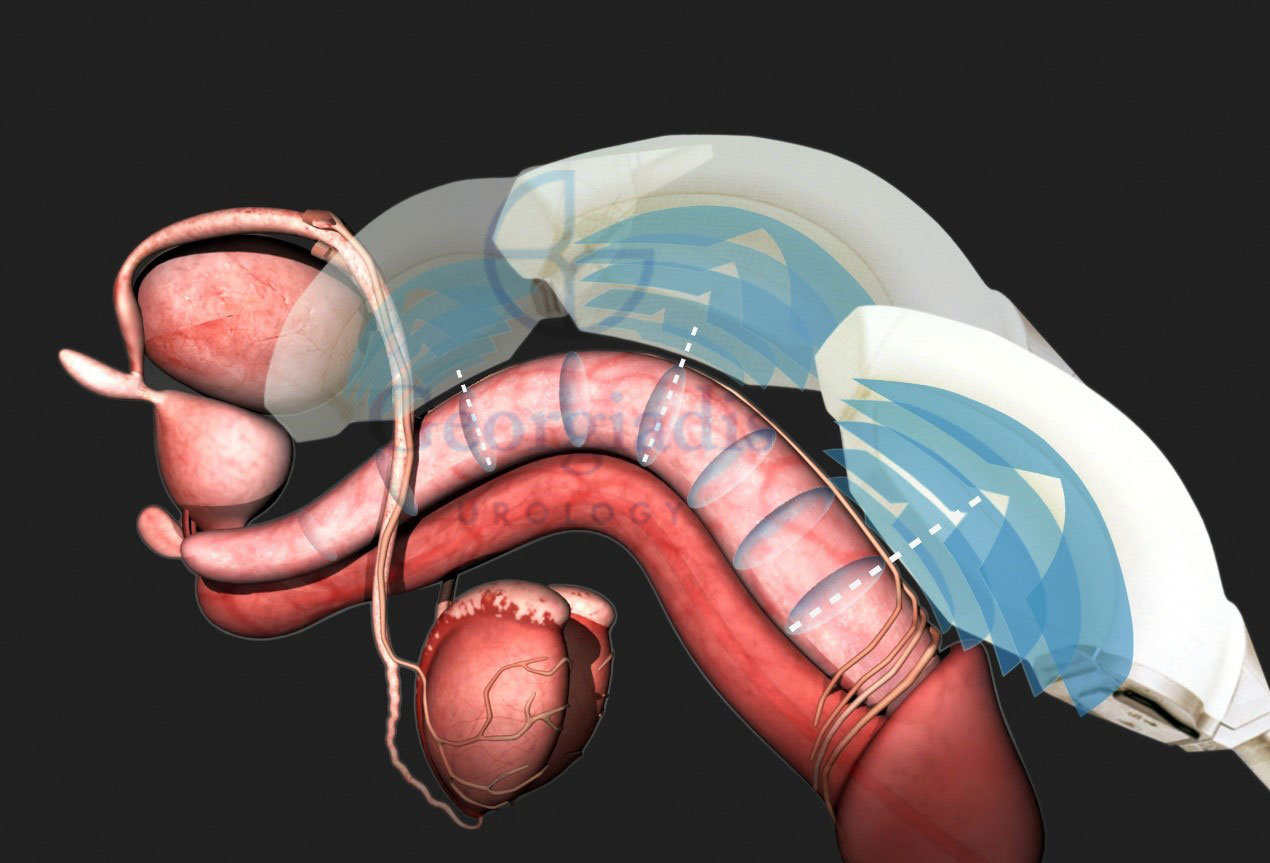
Figure 2: There is significant research backing the effectiveness of using low-intensity shockwave treatment for erectile dysfunction and this is why it is a part of GERP. At the same time, there is some criticism about its effectiveness waning after a few years, but in truth it is the fact that the majority of doctors do not know how to diagnose or treat the underlying Chronic Prostatitis, hence the effectiveness of shockwaves gradually decreases.
4. Platelet-rich Plasma (PRP) Therapy
Platelet-rich plasma therapy, also known as P-shot, refers to the injection of certain growth factors directly in the tissue (i.e. the penile tissue in our case), with the aim of initiating, multiplying and promoting the healing and regeneration of cells. It works by isolating and concentraing plasma, taken from the body’s blood through centrifugation, resulting in some special factors or proteins with the aforementioned beneficial effects.
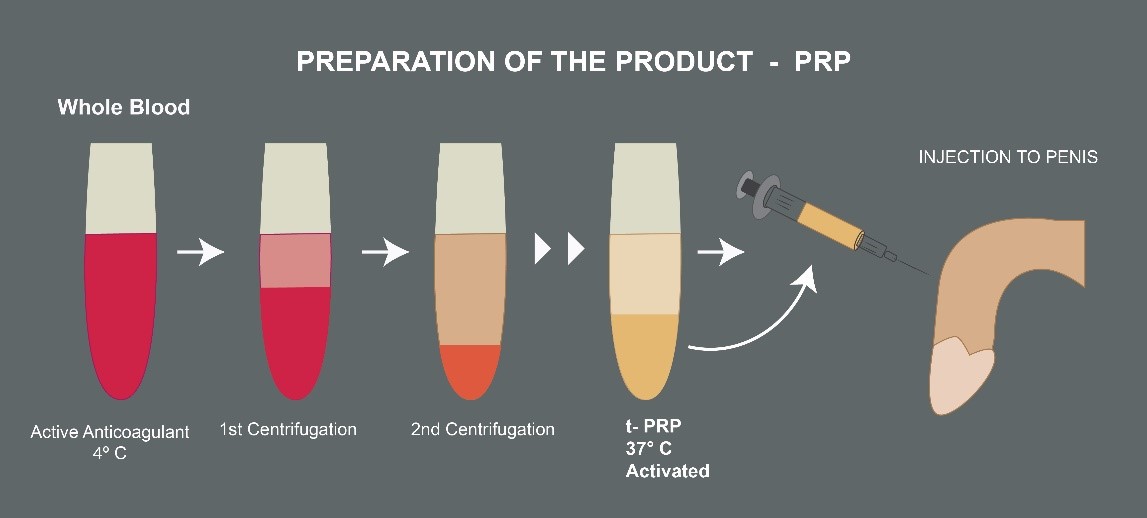
Figure 3: Starting from whole blood samples, we generate PRP, which is rich in growth factors through centrifugation. PRP injections are used in combination with the rest of the GERP protocol for the task of restoring the erectile function.
The total number of necessary P-shots (PRP therapies) depends on a number of factors:
- The patient’s penile tissue damage.
- The causal factor for the progressive penile cavernosal tissue fibrotic transformation, which is primarily chronic prostatitis.
- Additional conditions, which could aggravate the existing penile fibrotic status (e.g. diabetes, hypertension, high cholesterol etc.).
In the Georgiadis protocol, P-shots are usually done directly into the penile damaged cavernosal tissue, for 3 to 6 times, with an interval of 4-6 weeks between each time.
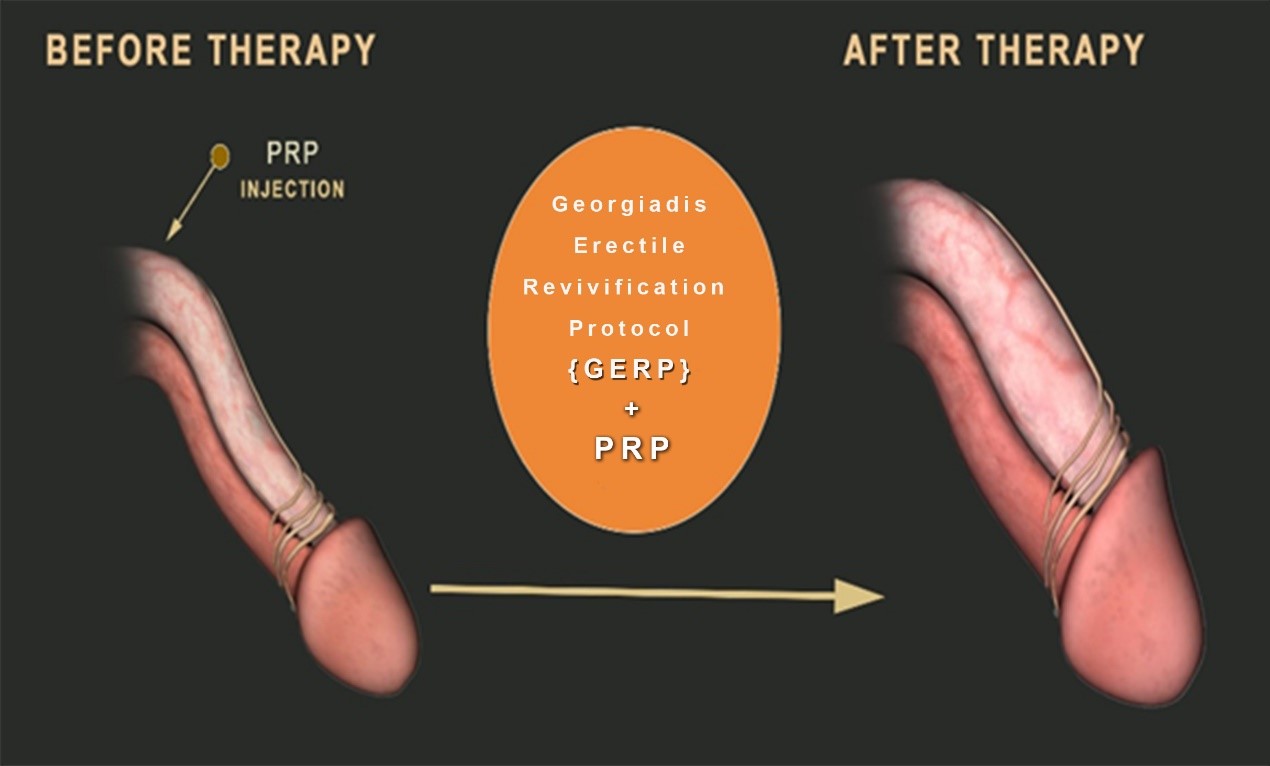
Figure 4: Graphical representation of the effect of PRP injections into the penile cavernosal corporal tissue during the “Georgiadis Erectile Revivification Protocol” (GERP). P-shots can effectively change the appearance of external male genitalia.
GERP Treatment Frequency
By combining the three aforementinoed techniques simultaneously, we practically perform a “reviving physiotherapy” of the penile tissue and its arterial micro-circulation. Typically, the frequency of GERP treatments in my protocol is three times per week:
- For 6-8 weeks, which is for mild cases (i.e. low chronicity that have had erectile dysfunction for less than one year).
- For up to 12-16 weeks for more severe cases (i.e. cases that have had the erectile dysfunction symptom for more than two years).
The results are very promising as about 90% of my patients report significant improvement after going through GERP. That being said, patients should always remember that they first need to treat their Chronic Prostatitis, otherwise:
- There may be zero improvement in their erectile dysfunction.
- Even if there is any improvement, it will only be temporary.
Multifactorial Erectile Dysfunction
In cases where we have to deal with other serious comorbidities (i.e. conditions occuring alongside ED) and lifestyle aggravating factors (e.g. obesity, smoking, drinking etc.), the success rate of GERP (i.e. number of patients noticing singificant improvement in ED) is empirically about 70%. This improvement may last for about two years or even longer, but the patient will have to also contribute in lifestyle changes (e.g. diet, cut unhealhty habits like heavy alcohol or smoking etc.) as well as preserve other comorbidities (e.g. diabetes) under control in order to make the effect long-lasting.
Lifestyle Changes
Many men with ED are able to improve their sexual function by making a few lifestyle changes. For example:
- Giving up smoking
- Losing weight
- Exercising more often
- Eating responsibly (i.e. low carbohydrates, high amount of vetables, avoiding sugars and spicies)
- Practicing safe sexual intercourse
While these changes are not enough to create a significant impact on their own, they constitute a part of the Georgiadis Erectile Revivifaction Protocol (GERP), as they can definitely speed it up.
Erectile Pills
Erectile pills like Viagra, Cialis, Levitra, Staxyn, Stendra etc. along with many other which contain natural vasoactive agents, all work by increasing blood flow to the penis during arousal. They’re generally taken 1 to 3 hours before sexual activity and should not be used more than once a day. Older men, and especially those having other medical issues (e.g. heart problems, high blood pressure etc.), all require an approval from the doctor for their safety before taking them.
Important note: As we have explained, patients who have erectile dysfunction actually suffer from an underlying cause – taking a pill is not a solution, it merely tries to address a symptom. The cause is, in the overwhelming majority of cases, a chronic inflammatory disease in the prostate, and as such taking those pills will lead to further worsening of ED, despite the initial temporary improvement.
In my experience, using erectile pills without treating the root cause is not only ineffective as a treatment for the symptom, but the inflammation gets more aggravated too. As a rule of thumb, when patients start using erectile pills, it is a good indication to go to a urologist to check for Chronic Prostatitis.
Psychological Factors
Treating erectile dysfunction from purely a psychological perspective (and not as an organic disease) is not only ineffective, it is also irresponsible. Leaving the organic factors untreated simply leads to a worsening of the situation, which further enhances the negative psychological impact of the disease on the patient.
The various psychological factors that may affect erectile dysfunction (e.g. stress, performance anxiety etc.) are typically vastly improved as the therapies for CP and ED progress and the patients start seeing the results.
Conclusion
To sum up, in order to treat erectile dysfunction, the patient has to:
- Cure the cause, which is chronic prostatitis (Georgiadis Chronic Prostatitis Protocol).
- Treat the complication (symptom), which is erectile dysfunction (Georgiadis Erectile Revivification Protocol).
- Manage any other conditions (e.g. diabetes, obesity, smoking etc.) that may affect their overall health.
